
URBAN ZOO PROJECT: The 99 Household Study
URBAN ZOO PROJECT: The 99 Household Study
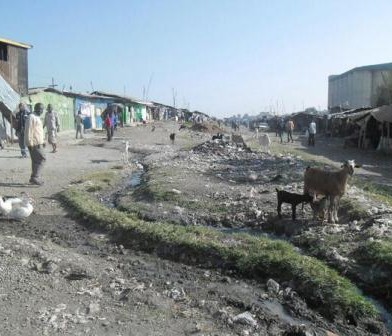
The 99 households study is now well under way, with sampling being carried out across a range of neighbourhoods in Nairobi. Each week the team targets a different sub-location, where three house-holds are recruited; two with different types of livestock and a third which does not keep any livestock species. Our team of clinical officers and vets collect samples from all human members of the house-hold, along with samples from livestock present, from the general household environment and from any animal source foods in the home. In addition, the wildlife team trap and sample rodents, wild birds, bats, primates and small carnivores in the vicinity.
Sampling a household is intensive, and participants not only consent to donate their faeces to the study, but also give up a good portion of their time, answering questionnaires, aiding the sampling by handling their livestock, and providing access to their property at all hours to allow checking of rodent traps. As such, only three households are sampled in a week, but after 8 weeks more than 400 samples have already been collected.
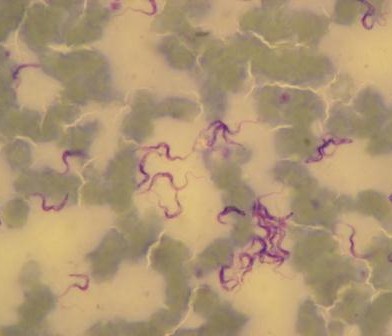
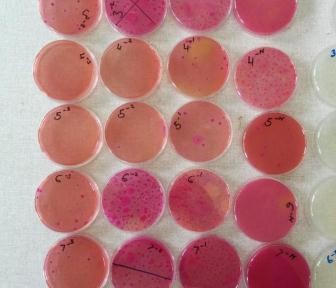
All samples are sent to our two collaborating laboratories at KEMRI and the University of Nairobi, where they are cultured to grow E.coli bacteria, the primary focus of the study. Multiple individual bacterial colonies are selected from the first culture to go forward for purification and further testing. This means that each animal, human or environmental sample taken in the field can generate up to five subsequent bacterial isolates, and so the number of colonies in the collection is increasing rapidly.
Genetic data from the bacterial samples will allow us to study similarities and differences between these normal bacteria carried by individuals, and how they can be shared between humans, animals and the environment. The questionnaire data collected, among other things, builds on the project’s previous work on value chains, and will allow us to assess how these consumers from a range of social strata are connected to the various value chains that exist in Nairobi for meat and animal products.
A great deal of work has led up to the start of this study, including developing strate-gies for finding participants to represent a diverse section of the city, developing sampling and laboratory protocols, and designing the electronic data capture sys-tems used in the field and laboratories. Everyone involved is delighted that things are now up and running and our colleagues in the UK are eagerly waiting for the first shipment of bacterial DNA to arrive. Watch our blog space!
This article has been written by Judy Bettridge (Post Doc under the 99HH Study, based jointly between the University of Liverpool, UK and International Livestock Research Institute (ILRI) in Kenya).

Using tablet to collect data

Sampling a rabbit in Makongeni

Field team in one of the sampling sites

Sampling the environment

Microbiology plates in readiness for culturing samples

















































You must be logged in to post a comment.